An article by Dr. Pauline Chen sums this up nicely with her quote, “An older nurse finally pulled me aside. ‘Just admit him,’ she whispered, ‘It’ll cost more, but it’s the only way you’ll be sure he’s getting the right care.’” There is a better way.1
Common Reasons for Presentation in the Older Adult Population

What is the Scope of the Issue?
In 2017 the US Department of Health and Human services reported a cost of ED visits estimated around ~$76 billion. The highest cost per visit was for patients over the age of 65. The majority of ED patients are treated and released and not hospitalized.2-3
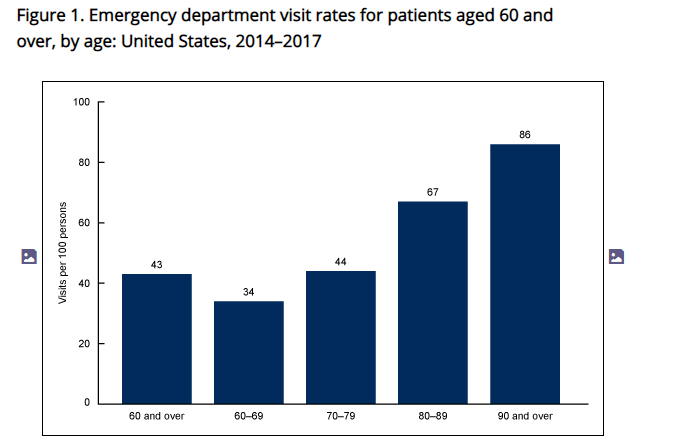
The CDC reports high visit rates for the adult population as shown below.3
Falls related ED visits are responsible for a huge financial toll and affect 1 in 4 Americans over the age of 65 each year. 20% of ED visits are related to falls alone.4-6 Just based on this data alone, EDs need to be prepared to better care for our older adult population.
Current Recommendations
The American College of Emergency Physicians offers a Geriatric accreditation program to ensure older adults are receiving optimal care while in Emergency Departments. This accreditation program ensures that best practices for the older adult population are met. A sample of these best practices include: appropriate education and interdisciplinary staffing, identify and provide standardized care approaches, ensure optimal transitions of care, and more. You can read all of the criteria and guidelines here.7
That’s Great, But What Can I Do?
If you work in a facility that is not GEDA Accredited and may not become accredited, there are many steps you can take to immediately begin improving care for your older adult patients.
For Administrators
If you do not already have rehab services embedded in your Emergency Department, now is the time to do so. There is extensive literature support for physical therapists as part of the ED team and evidence around occupational therapists in this department continues to emerge.
Physical therapists help reduce recidivism, unnecessary imaging, unnecessary hospital admissions, improve patient satisfaction, and assist in safe discharge planning.8-10 You can see our comprehensive reference list here. Occupational therapists are instrumental in prevention of delirium, assessment of ADL function, and cognition among many other skills. With the older adult population, these assessments are critical to ensure patients are being well-cared for and receiving the follow up resources needed.
Your rehab services team can also make recommendations about environmental considerations, fall risk reduction in the department, and staff training to improve patient care.
If you are ready to start an ED PT program, reach out – we can get you started on target.
For Physical Therapists
When working with the older adult population, ensure you are familiar with how these patients may differ from the younger population. Red flags are different, understanding of poly-pharmacy is essential, completing a comprehensive systems review is necessary. All of these components will inform your interventions and discharge planning.
If you feel like you need to brush up on these skills, consider our self-paced 3-hour webinar on Examination and Evaluation of the Older Adult in the Emergency Department. Contact me for 20% after mentioning this post.
Conclusion
Older adults make up a large percentage of patients in the Emergency Deparment. The addition of rehab services in the ED as part of the inter-disciplinary team in addition to awareness and implementation of best practices can improve care for older adults. Let’s work together to make the ED safe and accommodating for all of our patients.
Related Articles & References
- https://archive.nytimes.com/well.blogs.nytimes.com/2014/03/13/emergency-rooms-are-no-place-for-the-elderly/
- Moore BJ, Liang L. Cost of Emergency Department Visits in the United States, 2017. Agency for Healthcare Research and Quality. Dec 2020. Statistical Brief #268. https://www.hcup-us.ahrq.gov/reports/statbriefs/sb268-ED-Costs-2017.pdf
- U.S. Department of Health and Human Services Office of the Assistant Secretary for Planning and Evaluation. Trends in the Utilization of Demergency Services, 2009-2018. March 2, 2021. https://aspe.hhs.gov/system/files/pdf/265086/ED-report-to-Congress.pdf
- Get The Facts on Falls. https://www.ncoa.org/news/resources-for-reporters/get-the-facts/falls-prevention-facts/#:~:text=According%20to%20the%20U.S.%20Centers,adult%20dies%20from%20a%20fall.. Accessed March 202.
- Important Facts About Falls. https://www.cdc.gov/HomeandRecreationalSafety/Falls/adultfalls.html. Accessed March, 2021.
- Physical Therapy Guide to Falls. https://www.choosept.com/symptomsconditionsdetail/physical-therapy-guide-to-falls#WhatIs. Accessed March, 2021.
- https://www.acep.org/geda/
- Falvey JR, Burke JE, Stevens-Lapsley JE. Role of Physical Therapists in Reducing Hospital Readmissions: Optimizing Outcomes for Older Adults During Care Transitions from Hospital to Community. Physical Therapy. 2016 Aug; 96)8): 1125-1134.
- Russell MA, Hill KD, Day LM, Blackberry I, Schwartz J, Guimmarra MJ, Dorevitch M, Ibrahim JE, Dalton AC, Dharmage SC. A randomized controlled trial of a multifactorial falls prevention intervention for older fallers presenting to emergency departments. J Am Geriatr Soc. 2010 Dec;58(12):2265-74.
- Lesser A, Israni J, Kent T, Ko KJ. Association Between Physical Therapy in the Emergency Department and Emergency Department Revisits for Older Adult Fallers: A Nationally Representative Analysis. J Am Geriatr Soc. 2018 Nov;66(11):2205-2212. doi: 10.1111/jgs.15469. Epub 2018 Aug 21. PMID: 30132800