
By Seth Peterson, PT, DPT1; Rebekah Griffith, PT, DPT2; Mark Milligan, PT, DPT3
ABSTRACT
Each year millions of patients present to the emergency department (ED) for musculoskeletal pain making it one of the most common reasons for people to seek care in this setting. It is also no secret that EDs continue to be overburdened. Physical therapists (PT) have been positioned in many EDs with great impact and success which is a good first step to improve care, cost, and satisfaction. However, by moving further upstream, physical therapists can be the right provider at the right time to prevent or limit presentation to the ED when unnecessary for musculoskeletal complaints.
Following the COVID-19 pandemic, we learned many lessons about how to leverage telehealth to serve our patients by decreasing barriers to care. In 2021, a call to action suggested several ways to use digital health to expand access to care outside of the ED. This perspective will explain how digital triage by a PT could safely and effectively reduce the number of patients presenting to an ED for non-emergent musculoskeletal conditions. Digital physical therapist triage would not only prevent patients with pain or movement impairments from inappropriately seeking emergency care but could also increase early access to ongoing physical therapist management.
“It was the worst experience of my life,” said a petite 79-year-old woman, and patient of one of the authors, of her recent experience in the emergency department (ED). Over the weekend, she had developed severe radiating leg pain. Perceiving it as a serious problem, she went to the ED. There, she spent 12 hours unattended in a hospital hallway. Eventually, she had her blood drawn and received an anticoagulant injection because she had been waiting so long. Since there was a delay for imaging, she was admitted, and when she finally had images taken, they were for her neck rather than her back. Four days later, she reflected on the dehumanizing experience with a shudder of apprehension for the large medical bill looming in her future.
It is no secret that emergency care in the United States needs help. Overcrowding in the ED is a major healthcare concern and a contributor to scenarios where “too much” or “not enough” care is administered.1, 2 It is estimated that over 9 million patients present to the ED each year for musculoskeletal pain,3 making it one of the most common reasons people seek care in the ED. However, nearly half of these visits are unnecessary,4 which is a concern given that these patients often endure long wait times,5 crowded environments, and large medical bills. Positioning physical therapists in the ED can reduce wait times, unnecessary imaging, and opioid prescriptions6; and it may even improve patient and provider satisfaction.7-9 By having a presence in the ED, physical therapists can also provide immediate treatment and facilitate appropriate follow-up care, which leads to better patient outcomes.10
For decades, physical therapists all over the world have been successfully positioned in the ED.11-13 Along came the COVID-19 pandemic, which resulted in severe access issues for emergency, urgent, and routine care. Suddenly, everyone became familiar with hospital problems such as overcrowding and bedlock.14 In response, many EDs expanded their personnel rosters with other healthcare professionals, such as nurse practitioners, physician assistants, social workers, case managers, and rehabilitation professionals—including physical therapists.15
The COVID-19 pandemic also accelerated the use of telehealth as barriers to its implementation seemed to evaporate overnight. In 2021, a call to action suggested several ways that digital health could be used to expand access to emergency care outside the ED through a “virtual ED.”16 The authors reported results of synchronous telemedicine calls in their hospital systems, where only 5%-10% of visits were referred to the ED.16 Given the value of physical therapists to the in-person ED, it is worth considering the value that they could offer to one that was virtual. However, although positioning physical therapists in the ED is a good first step to improve care, cost, and satisfaction, we suggest a model that is even further upstream—digital physical therapist triage. For this digital health model, physical therapists outside the emergency setting can consult with patients who are unsure whether a visit to the ED is even necessary. In this perspective report, we will explain how digital physical therapist triage could work and how physical therapists could safely and effectively implement such a program.
GETTING OUT FRONT: DIGITAL PHYSICAL THERAPIST TRIAGE
The role of physical therapists has changed substantially over the past 50 years. Today, physical therapists across the world have advanced practice roles and are responsible for decision-making about diagnosis and referral.17 Further, positioning physical therapists at the point of entry into care has been wildly successful in the United States military, improving patient safety, access, efficiency, satisfaction, and cost savings.18 It may be possible to emulate such a model virtually, especially since musculoskeletal pain is an extremely common reason to seek care in the ED,3 physical therapists rank highly in their musculoskeletal knowledge,19 and there is significant agreement between physical therapists and ED physicians in terms of diagnosis and treatment plans.20
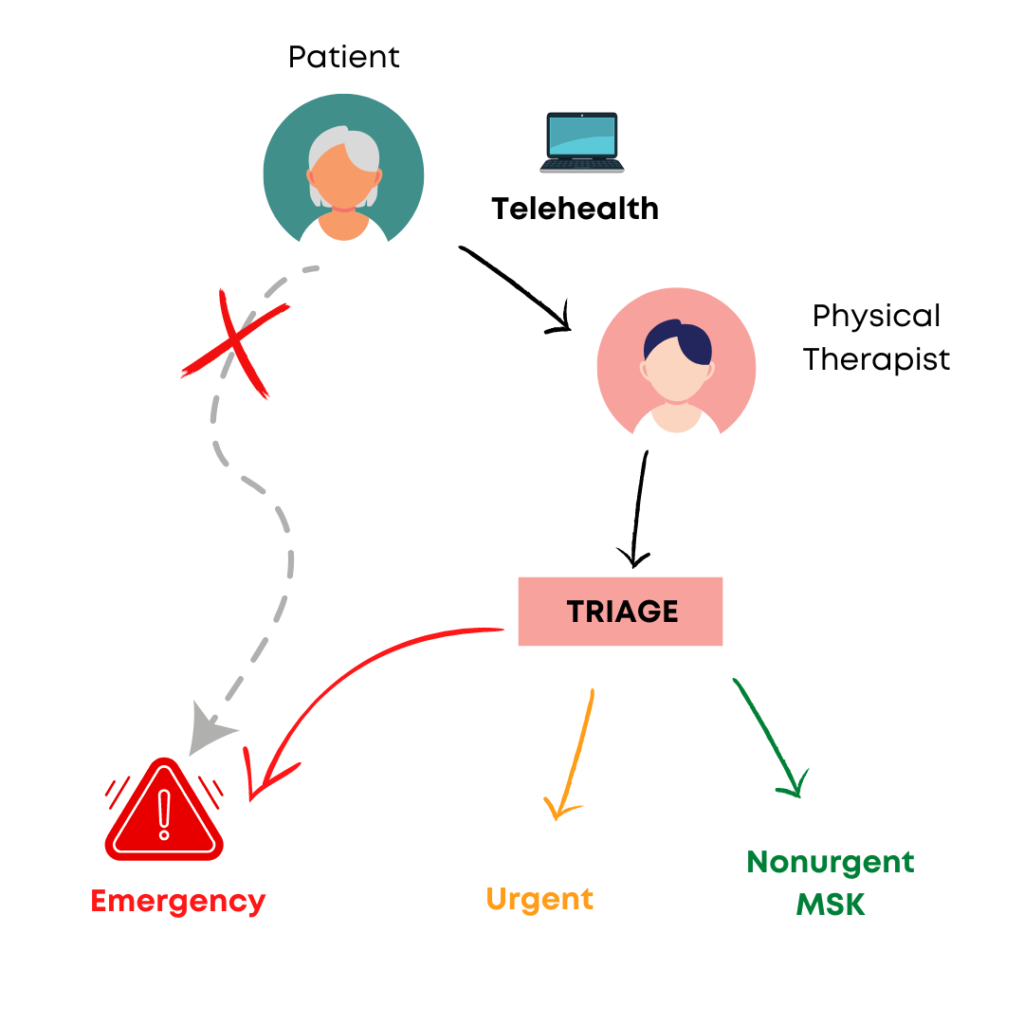
Given the low number of patients with musculoskeletal pain who actually require emergency care, digital access may provide an option for physical therapists to get involved with triage of patients through the “input” phase. In other words, if emergency virtual appointments are made available, patients with musculoskeletal pain or movement impairments who are considering whether to seek care in the ED could consult physical therapists and, thus, be directed toward appropriate medical channels (Figure 1). For example, the 79-year-old woman with radiating leg pain from the beginning of this report could have immediately consulted with her physical therapist in her home, received education and exercise to improve her symptoms, or perhaps been directed to an outpatient physical therapy clinic, thereby saving her a large medical bill and lightening the load on the local ED. Digital physical therapist triage would not only prevent patients with pain or movement impairments from inappropriately seeking emergency care, but could also establish a more thoughtful follow-up plan for these patients and increase early access to ongoing physical therapist management.
EXECUTING DIGITAL PHYSICAL THERAPIST TRIAGE: CHALLENGES AND OPPORTUNITIES
Digital physical therapist triage may also involve more challenging scenarios. In such instances, the physical therapist’s clinical reasoning should follow the same process used during a typical patient evaluation. As part of their reasoning, physical therapists must determine whether the scenario is nonurgent, urgent, or emergent and then act accordingly. Ideally, the triage process develops by establishing an overall level of concern given the patient profile, salient features, and consequence of delay.21 Although it may be difficult to perform some physical examination testing during digital physical therapist triage, such factors should be considered when making decisions about diagnosis and referral since they may introduce uncertainty.
One example of an “urgent” scenario would be an older patient who may need to be evaluated for a hip fracture after a fall. If a fracture is suspected, physical therapists in many states can directly refer for the necessary imaging. For physical therapists in states not afforded imaging privileges, they are still able to facilitate an urgent referral to an urgent care center, the patient’s primary care physician, or elsewhere. Although possible, this action requires additional effort on the part of the physical therapist, which we believe is further evidence that barriers to imaging arbitrarily impede patient access to efficient models of care based solely on the patient’s state.
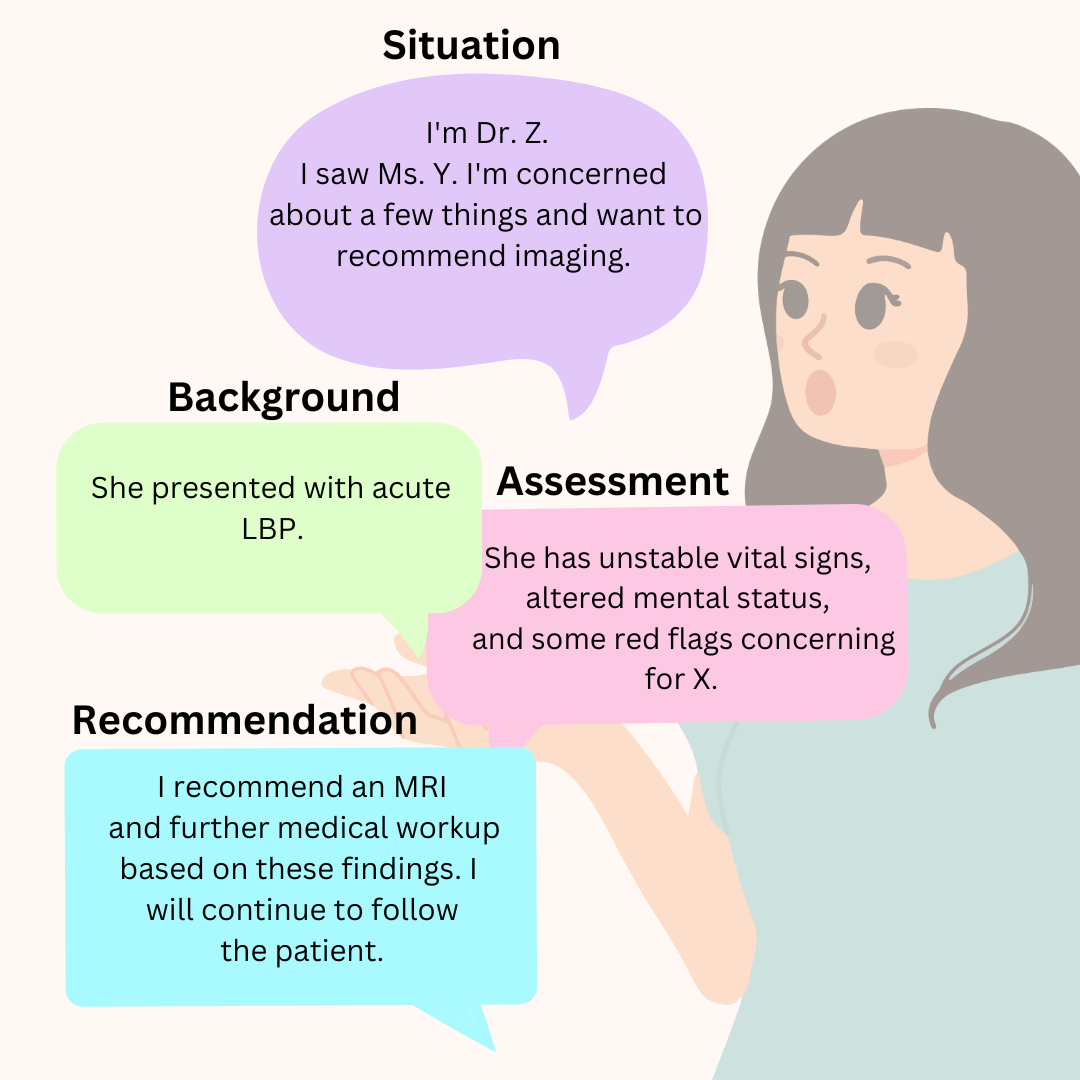
Occasionally, those implementing digital physical therapist triage may encounter patients who do require an emergency referral. Because patients sometimes have problems with transportation and access to the ED,22 the physical therapist could serve a role by directing them to the most appropriate location and facilitating appropriate and safe transportation. Physical therapists could also spend time ensuring that care continuity is established with the patient’s primary care physician and the ED. Such continuity could occur through verbal or written communication using the “SBAR” format to alert the ED of the situation, background, assessment, and recommendation. An example of an emergency scenario communicated using the SBAR format is presented in Figure 2.
However, there are challenges to implementing this model in practice. As described above, directing some patients to the appropriate medical channels requires the physical therapist to have a high degree of comfort making decisions about diagnosis and referral, which may be unrealistic for some. Further, those who decide to implement such a program may require additional training on these topics and how to effectively use telehealth. Since a greater variety of clinical conditions may present during digital physical therapist triage, there may also be some increased risk, which may dissuade some clinics from developing and implementing such programs. However, we do not believe the direct nature of access will be a major barrier to implementation because most states already have direct access and are therefore already receiving some patients who require emergency referral. Finally, when physical therapists insert themselves into the “input” phase of emergency care, they have to make time available to evaluate these patients and coordinate their care, which is a barrier given tight clinic schedules. One solution to this problem is to have dedicated time slots each day for digital physical therapist triage; however, each clinic will need to determine what works best for their business and their communities.
CONCLUSION
Digital physical therapist triage has the potential to decrease unnecessary ED visits, thereby reducing costs, improving health, and raising patient satisfaction. Physical therapists have been valuable team members in emergency care for decades. Therefore, as EDs consider expanding emergency care through technology, physical therapists should continue to look boldly into the future and determine how their skills can be best used to serve patients in their communities. After all, perhaps the greatest advantage of telehealth is not only the opportunity to replicate care already available in person, but to also allow for the creation of models of care that would otherwise be impossible to imagine.
To learn more click here.
REFERENCES
1. Sandhu P, Shah AB, Ahmad FB, et al. Emergency department and intensive care unit overcrowding and ventilator shortages in US hospitals during the COVID-19 pandemic, 2020-2021. Public Health Rep. 2022;137(4):796-802. doi:10.1177/00333549221091781
2. Núñez A, Sreeganga SD, Ramaprasad A. Access to healthcare during COVID-19. Int J Environ Res Public Health. 2021;18(6):2980. doi:10.3390/ijerph18062980
3. Cairns C, Kang K, Santo L. National Hospital Ambulatory Medical Care Survey: 2018 emergency department summary tables. Centers for Disease Control and Prevention. Accessed January 10, 2023. https://www.cdc.gov/nchs/data/nhamcs/web_tables/2018-ed-web-tables-508.pdf
4. Gaieski DF, Mehta S, Hollander JE, Shofer F, Bernstein J. Low-severity musculoskeletal complaints evaluated in the emergency department. Clin Orthop Relat Res. 2008;466(8):1987-1995. doi:10.1007/s11999-008-0277-5
5. Horwitz LI, Green J, Bradley EH. US emergency department performance on wait time and length of visit. Ann Emerg Med. 2010;55(2):133-141. doi:10.1016/j.annemergmed.2009.07.023
6. Pugh A, Roper K, Magel J, et al. Dedicated emergency department physical therapy is associated with reduced imaging, opioid administration, and length of stay: a prospective observational study. PLoS One. 2020;15(4):e0231476. doi:10.1371/journal.pone.0231476
7. Sheppard LA, Anaf S, Gordon J. Patient satisfaction with physiotherapy in the emergency department. Int Emerg Nurs. 2010;18(4):196-202. doi:10.1016/j.ienj.2009.11.008
8. Barrett R, Terry L. Patients’ and healthcare professionals’ experiences and perceptions of physiotherapy services in the emergency department: a qualitative systematic review. Int J Emerg Med. 2018;11:42. doi:10.1186/s12245-018-0201-z
9. Good DM. Emergency department physical therapy: an important tool for emergency physicians. Acad Emerg Med. 2021;28(8):936-937. doi:10.1111/acem.14300
10. Magel J, Kim J, Fritz JM, Freburger JK. Time between an emergency department visit and initiation of physical therapist intervention: health care utilization and costs. Phys Ther. 2020;100(10):1782-1792. doi:10.1093/ptj/pzaa100
11. Kempson SM. Physiotherapy in an accident and emergency department. Accid Emerg Nurs. 1996;4(4):198-202. doi:10.1016/s0965-2302(96)90081-8
12. Gill SD, Stella J. Implementation and performance evaluation of an emergency department primary practitioner physiotherapy service for patients with musculoskeletal conditions. Emerg Med Australas. 2013;25(6):558-564. doi:10.1111/1742-6723.12134
13. Morris CD, Hawes SJ. The value of accident and emergency based physiotherapy services. J Accid Emerg Med. 1996;13(2):111-113. doi:10.1136/emj.13.2.111
14. Janke AT, Melnick ER, Venkatesh AK. Hospital occupancy and emergency department boarding during the COVID-19 pandemic. JAMA Netw Open. 2022;5(9):e2233964. doi:10.1001/jamanetworkopen.2022.33964
15. Pontius EA, Anderson RS Jr. Physical therapy, occupational therapy, and speech language pathology in the emergency department: specialty consult services to enhance the care of older adults. Emerg Med Clin North Am. 2021;39(2):419-427. doi:10.1016/j.emc.2021.01.005
16. Hollander JE, Sharma R. The availabilists: emergency care without the emergency department. NEJM Catal Innov Care Deliv. Published December 21, 2021. Accessed January 10, 2023. https://catalyst.nejm.org/doi/full/10.1056/CAT.21.0310
17. Tawiah AK, Desmeules F, Finucane L, et al. Advanced practice in physiotherapy: a global survey. Physiotherapy. 2021;113:168-176. doi:10.1016/j.physio.2021.01.001
18. Clark B, Clark L, Showalter C, Stoner T. A call to action: direct access to physical therapy is highly successful in the US military. When will professional bodies, legislatures, and payors provide the same advantages to all US civilian physical therapists? J Man Manip Ther. 2022;30(4):199-206. doi:10.1080/10669817.2022.2099893
19. Childs JD, Whitman JM, Sizer PS, Pugia ML, Flynn TW, Delitto A. A description of physical therapists’ knowledge in managing musculoskeletal conditions. BMC Musculoskelet Disord. 2005;6:32. doi:10.1186/1471-2474-6-32
20. Matifat E, Perreault K, Roy JS, et al. Concordance between physiotherapists and physicians for care of patients with musculoskeletal disorders presenting to the emergency department. BMC Emerg Med. 2019;19:67. doi:10.1186/s12873-019-0277-7
21. Finucane LM, Downie A, Mercer C, et al. International framework for red flags for potential serious spinal pathologies. J Orthop Sports Phys Ther. 2020;50(7):350-372. doi:10.2519/jospt.2020.9971
22. Coster JE, Turner JK, Bradbury D, Cantrell A. Why do people choose emergency and urgent care services? A rapid review utilizing a systematic literature search and narrative synthesis. Acad Emerg Med. 2017;24(9):1137-1149. doi:10.1111/acem.13220

- Seth Peterson PT, DPT, The Motive Physical Therapy Specialists, Oro Valley, AZ, USA; and Department of Physical Therapy, Arizona School of Health Sciences, A.T. Still University, 5850 E. Still Circle, Mesa, AZ 85206, USA. Address all correspondence to Dr. Peterson at: srpeterson01@atsu.edu
- Rebekah Griffith PT, DPT, Inpatient Rehabilitation Therapy Department, University of Colorado Hospital, Aurora, CO, USA; Physical Therapy Program, Department of Physical Medicine and Rehabilitation, Aurora, CO, USA; and The ED DPT, Highlands Ranch, CO, USA.
- Mark Milligan PT, DPT, Vori Health, Nashville, TN; REvolution Human PT and ED, Austin, TX, USA; and Anywhere Healthcare, Austin, TX, USA.


